Many people think vision is an all-or-nothing experience; you either see or you don’t. In reality, vision exists on a continuum.
Between perfect sight and total blindness are many levels of visual ability, and this is where low vision lies. Visual impairment is the general term used for people whose vision is less than normal, with normal vision measured as 6/6 or 20/20. For many, spectacles, contact lenses, or surgery can restore vision to this level. However, there are individuals whose vision cannot be fully corrected even with the best available treatment. These individuals are described as partially sighted or, more precisely, as having low vision.
Low vision is not a disease. Just as blurred vision is a symptom rather than a diagnosis, low vision is the outcome of underlying eye conditions such as glaucoma, diabetic eye disease, macular degeneration, or advanced cataract. In some cases, the damage caused by these conditions is irreversible. When this happens, the person must live with reduced vision for life. Not all visual blur interferes with daily functioning, but when it does, it becomes a serious disability. Low vision can affect a person’s ability to walk safely, recognise faces, watch television, sort stones from grains, count money, use a mobile phone, read religious texts, or even read this article. Research from low vision rehabilitation settings, including work I have been involved in, consistently shows that these functional difficulties, not just reduced visual acuity, are what most profoundly affect quality of life.
The consequences can be devastating. People with low vision may lose their jobs, withdraw from social activities, and experience anxiety or depression. Relationships and independence are often strained. Worse still, because people with low vision can sometimes recognise faces or perform certain visual tasks, others may assume they are pretending or exaggerating their difficulties. This misunderstanding adds stigma to an already challenging condition.
Management
Low vision is a form of disability, and like many disabilities, it often requires rehabilitation rather than a cure. Low vision care focuses on helping individuals use their remaining vision more effectively to regain independence. This process may involve training, environmental modification, and the use of assistive devices such as magnifiers, telescopes, improved lighting, and mobile phone accessibility features. Studies from low vision clinics show that when patients receive structured rehabilitation, many regain the ability to read, manage finances, and perform daily tasks independently, sometimes for the first time since losing their vision.
In Ghana, low vision care is mainly provided by optometrists, often working alongside rehabilitation professionals and disability resource centres.
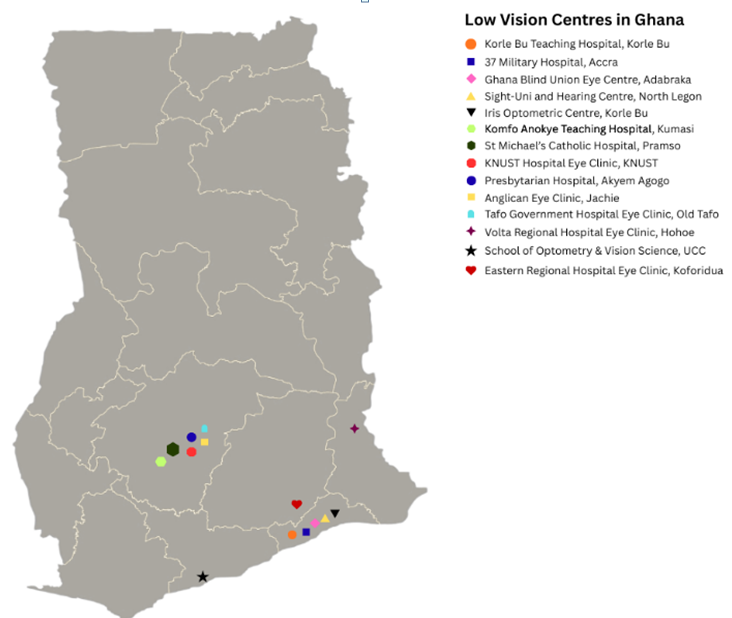
Where Can Low Vision Services Be Found?
The problem
Ghana has over 1.2 million people with varying levels of visual impairment, a significant proportion of whom have low vision. Global estimates always show that approximately half to two-thirds of those with visual impairment have low vision. People who are mostly affected are those aged 50 years and above. With the life expectancy in Ghana rapidly increasing and our world becoming more visual, it is likely that the demand for low vision services is bound to increase. However, there are very few low vision practitioners in the country and fewer centres that provide these services.
Major Challenges to Low Vision Care in Ghana
The low service coverage has been persistent due to multiple challenges. One major challenge is governance and funding. The Ghana Eye Care Secretariat, which coordinates eye care activities under the Ghana Health Service, relies heavily on donor funding. While this has supported valuable training initiatives, it limits long-term, sustainable development of low vision services.
Another challenge is the severe shortage and uneven distribution of trained low vision practitioners. Low vision care is time-intensive, often requiring one to two hours for an initial assessment. Poor remuneration and limited recognition of the sub-speciality discourage many optometrists from offering these services, despite the additional training required.
Awareness is also a major barrier. Many people with low vision do not know that help exists, and some eye care practitioners still underestimate the benefits of rehabilitation. To address this, the Ghana Optometric Association has designated February as Low Vision Awareness Month, aimed at educating both the public and professionals.
Cost remains a significant obstacle. Low vision devices are expensive, and many patients have already lost their source of income due to vision loss. Evidence from local clinics suggests that about six out of ten patients are unable to purchase prescribed low vision aids. None of these devices is currently covered under the National Health Insurance Scheme. Including even basic low vision aids under NHIS would dramatically improve access.
Finally, low vision care cannot succeed in isolation. Rehabilitation works best when supported by an inclusive society. Training someone to use public transport safely is meaningless if buses do not reserve seats for persons with disability, as required by the Ghana Disability Act. Buildings, roads, walkways, and public spaces must be designed with visual impairment in mind. Disability experts and persons with lived experience must be involved in planning and decision-making.
The Way Forward
To ensure people with low vision care and rehabilitation undergo the needed development to meet the growing demand, we must:
• Strengthen referral networks between hospitals, optometry clinics, and community-based rehabilitation services
• Integrate low vision services into primary healthcare and social protection systems
• Expand undergraduate and postgraduate training in low vision management
• Promote public–private partnerships to make assistive technologies affordable
• Involve low vision practitioners and persons with visual disabilities in policy design, implementation, and evaluation
Low vision can affect anyone through disease, injury, or ageing. None of us is immune. Building a system that supports people with low vision is not just an act of compassion; it is an investment in dignity, independence, and inclusion for all.
The writer, Dr Carl Halladay Abraham, is a lecturer, optometrist and low vision specialist at the School of Optometry and Vision Science, University of Cape Coast.
#Vision














Leave a Reply